Renal arterial resistive index identifies thrombotic microangiopathy after kidney xenotransplantation in pig-to-baboon model
Sho Fujiwara1, M. Esad Gunes1, Dominik Hajosi1,2, Olivia Sinn Kay Chan2, Kyosuke Chinuki1, David Berglund3, Erik Berglund4, Ibrahim Batal5, David H. Sachs1, Megan Sykes1, Greg Nowak1.
1Columbia Center for Translational Immunology, Columbia University, New York, NY, United States; 2Institute of Comparative Medicine, Columbia University, New York, NY, United States; 3Department of Immunology, Genetics and Pathology, Uppsala University, Uppsala, Sweden; 4Department of Molecular Medicine and Surgery, Karolinska Institute, Stockholm, Sweden; 5Department of Pathology, Columbia University, New York, NY, United States
Background: As kidney xenotransplantation (KXTx) advances toward clinical trials, the development of effective, non-invasive methods for graft monitoring becomes increasingly essential. Renal resistive index (RRI), derived from Doppler ultrasound sonography (DUS), is widely utilized in kidney allotransplantation to assess graft dysfunction and detect rejection episodes. However, its applicability in KXTx, particularly in identifying thrombotic microangiopathy (TMA), a frequent and severe complication leading to graft loss, has not been thoroughly investigated. This study assesses the potential of RRI as an early predictive indicator of TMA in a pig-to-baboon kidney xenotransplantation model.
Methods: Five consecutive pig-to-baboon KXTx were included in this prospective study. The first three cases comprised the study group (n=3), while the subsequent two served as a validation group (n=2). Serial RRI measurements were performed and compared with histopathological findings from kidney biopsies, either taken concurrently with ultrasound examinations or at the subsequent biopsy following RRI assessment. Renal artery RRI measurements from naïve pigs (n=8) and naïve baboons (n=6) were utilized as baseline reference values.
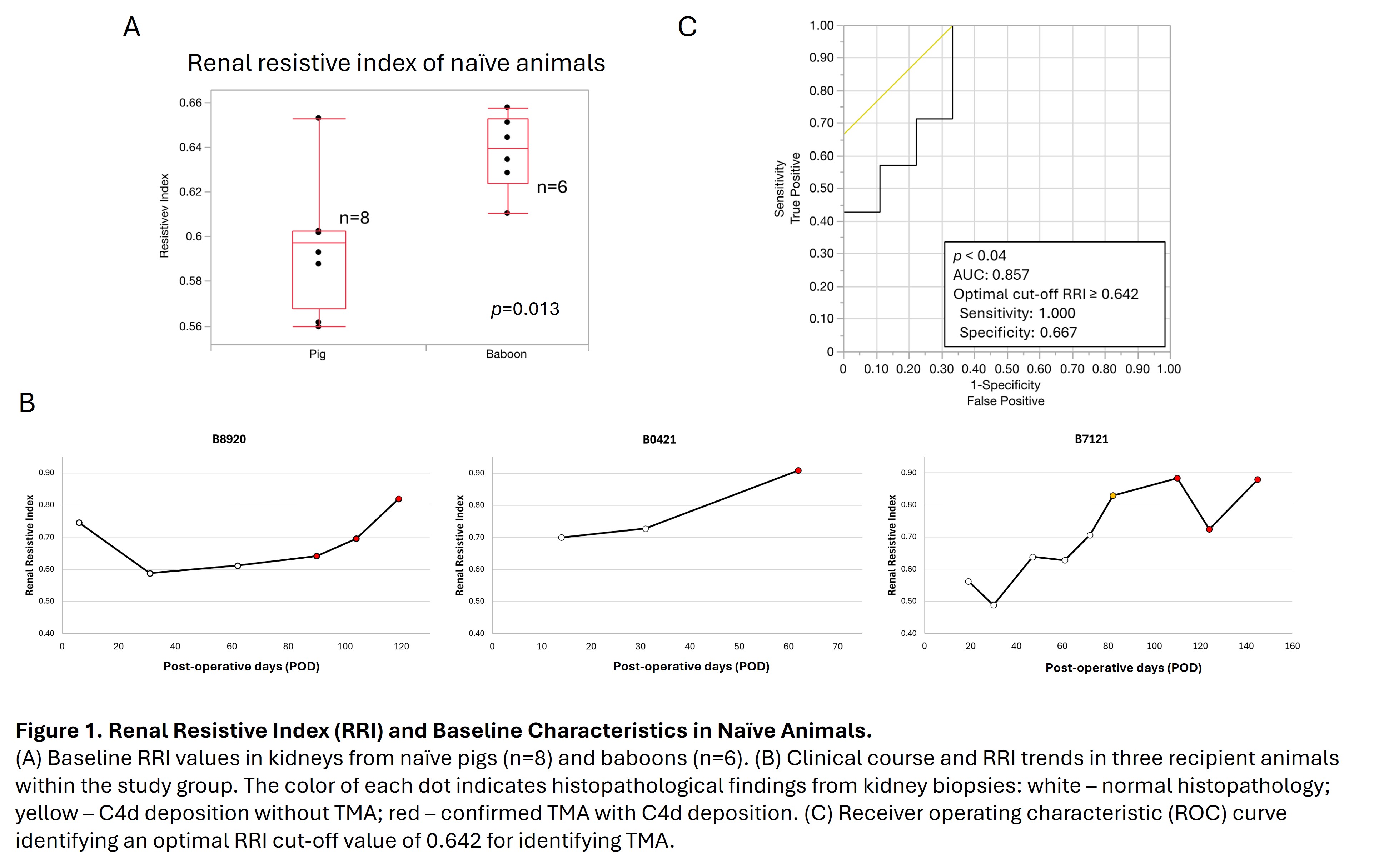
Results: Baseline RRI values were significantly lower in the kidneys of naïve pigs compared to naïve baboons (median [IQR]: 0.597 [0.568–0.603] vs 0.640 [0.624–0.653], respectively; p<0.02). In the study group, elevated RRI values were observed at the time when TMA was confirmed by biopsy (median [IQR]: 0.820 [0.696–0.883] vs 0.628 [0.575–0.717], respectively; p<0.02). The optimal RRI cut-off value associated with TMA following KXTx was 0.642 (ROC AUC=0.857, p<0.04), with a sensitivity of 1.000 and specificity of 0.667.
In the validation group, RRI transiently increased above 0.70 immediately following reperfusion but subsequently declined to pre-transplant baseline levels within one week post-transplantation (0.50 and 0.48, respectively). However, on POD 17 and 19, the RRI again increased beyond the critical threshold of 0.642, measuring 0.71 and 0.66, respectively, despite normal serum creatinine levels. Biopsies performed at these time points indicated a suspicion of TMA without accompanying renal dysfunction, and subsequent biopsies confirmed TMA on POD 21 and 22, respectively.
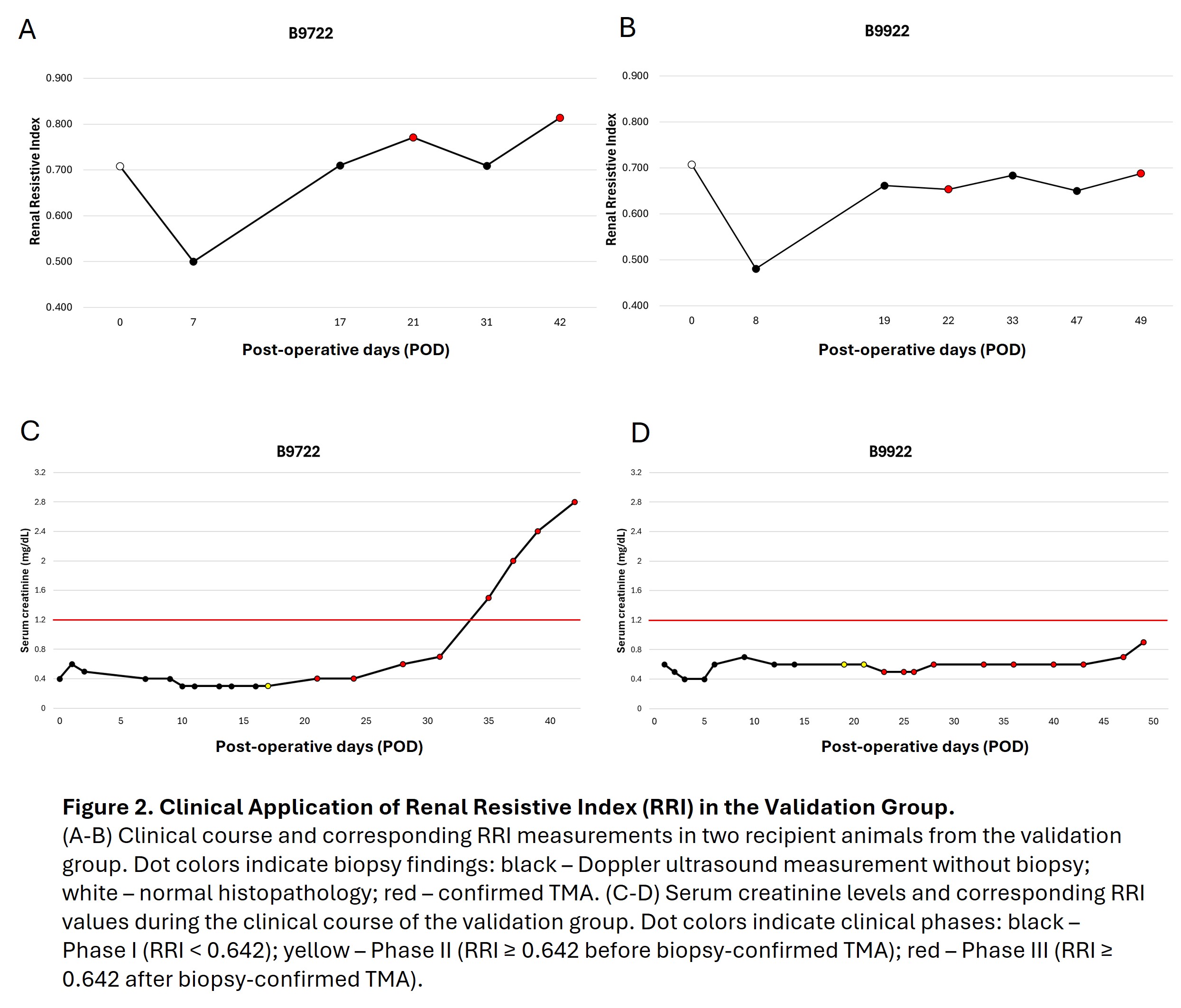
Conclusion: This study suggests that non-invasive DUS-based RRI measurement may be a sensitive method for the early detection of commonly diagnosed TMA in kidney xenografts. An RRI value above 0.642 effectively identifies the onset of TMA, even when serum creatinine levels remain within normal ranges, indicating no apparent renal dysfunction. These results highlight the potential of RRI as a valuable monitoring tool for KXTx, potentially enabling early identification of graft complications and timely interventions that could prevent graft loss. Further research is warranted to validate the utility of RRI as a reliable biomarker in clinical xenotransplantation.
This project was funded by the National Institute of Health (NIH) 5P01AI045897 grant and an unrestricted research grant from Nefro Health and ChoironeX.
[1] Kidney xenotransplantation
[2] Doppler ultrasound sonography
[3] Renal resistive index
[4] Thrombotic microangiopathy