Invasive versus echocardiographic hemodynamics in two genetically modified porcine to human cardiac xenotransplants
Alice Tang1, Muhammad Mohiuddin2, Cullen Soares1,4, Susie Hong-Zohlman1, Andrew Tully2, Javier Galindo2, Marco Oldsman1, Sarah Cipriano1, Timm Dickfeld1, Brian Barr1, Sadegh Asadi1, Anuj Gupta1, Alison Grazioli2, Allison Lankford2, Erika Feller3, David Ayares5, Bartley Griffith2, Manjula Ananthram1.
1Cardiology, University of Maryland, Baltimore, MD, United States; 2Cardiac Surgery, University of Maryland, Baltimore, MD, United States; 3Cardiology, Medstar Health, Bel Air, MD, United States; 4Cardiology, Tufts, Boston, MA, United States; 5National Heart, Lung, and Blood Institute, National Institute of Health, Bethesda, MD, United States
Background: Our institution performed two transgenic porcine to human cardiac xenotransplantations. There is limited data with the first cardiac xenograft suggesting echocardiographic assessment of the cardiac xenograft in humans correlates with invasive hemodynamic assessments. We investigated whether echocardiographic-derived hemodynamic indices would correlate with invasive measurements in both cardiac xenotransplants.
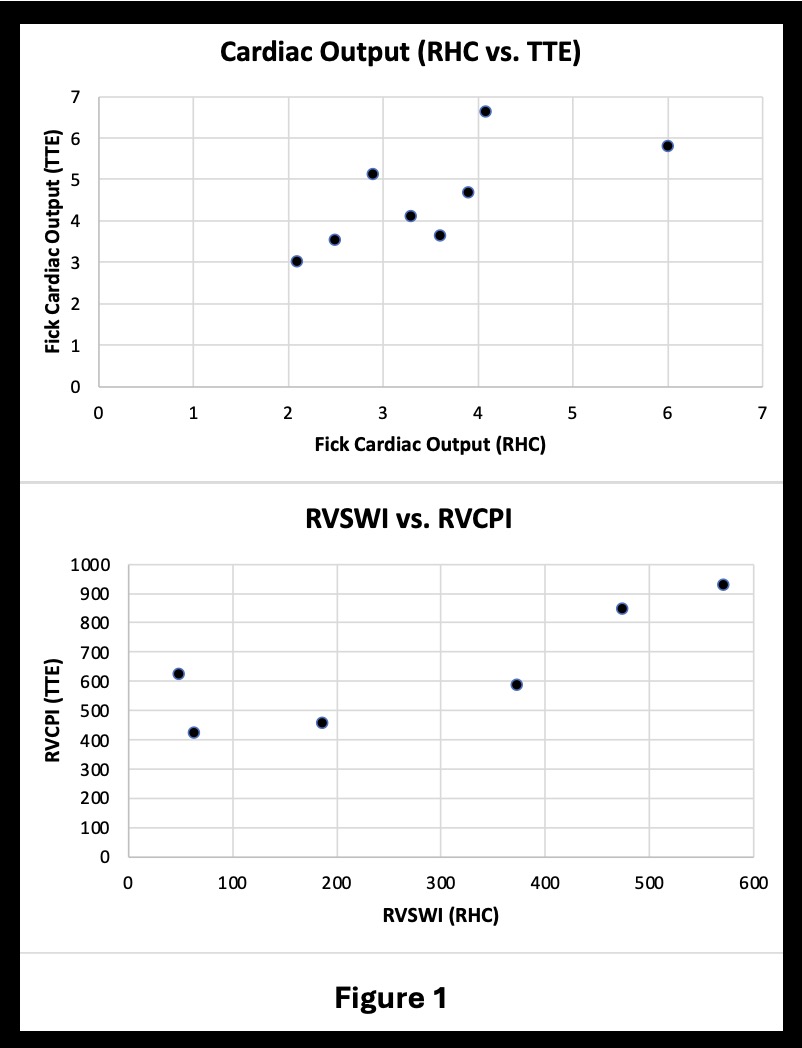
Methods: Serial transthoracic echocardiography (TTE) and right heart catheterizations (RHC) were performed in the cardiac xenografts. Retrospective analysis of TTE and invasive hemodynamics were analyzed in both the first and second xenotransplant to assess correlation between various parameters. Invasive hemodynamic measures include right atrial pressure (RAP), pulmonary artery systolic and diastolic pressures (PASP, PADP), Fick cardiac output (CO), cardiac index (CI), right ventricular stroke work index (RVSWI), and cardiac power output (CPO). TTE measurements and calculations included: RAP, PASP calculated via tricuspid regurgitation velocity (TRV), PADP based on end diastolic pressure gradient, tricuspid annular plane systolic excursion (TAPSE), right ventricular outflow time-velocity integral (TVI RVOT), pulmonary vascular resistance (PVR) = [TRV/TVI RVOT x 10 + 0.16], CO, CI, cardiac power output (CPO) = [mean arterial pressure echo-derived CO / 451], and right ventricular contraction pressure index (RVCPI) = [4x(TRV)²) x TAPSE], as a surrogate of RVSWI.
Results: Pearson correlation using invasive measurements at the time of TTE for cardiac output shows a positive correlation of 0.69 (p = 0.06) with a trend towards significance. Pearson’s correlation of RVSWI and RVCPI demonstrated a significant positive correlation of 0.83 (p = 0.04).
Conclusions: In the first two cardiac xenotransplants, there remains a positive correlation in hemodynamic markers between invasive and noninvasive measurements. Given the intense interest in cardiac xenotransplant, continued investigation in correlating noninvasive and invasive hemodynamic markers will provide real-time prognostic and clinical value for future research.
[1] Cardiac Xenotransplant